
Raise taxes or ration health care? Why single-payer won't work in California. Yet


Photo by Renée C. Byer, The Sacramento Bee
Betty Doumas-Toto's health insurance premium rose nearly 48 percent in January, to $800 per month for an Affordable Care Act plan. She and her husband are both Los Angeles freelancers in the film industry and are draining their savings trying to keep up with their monthly payments.
A Pomona mother of five named Claudia, who is undocumented, can't get health insurance because of her immigration status. She's losing her hearing, but can't afford tests a doctor ordered because the costs are too high.
At an elder care home in the Sacramento suburbs, small business owners Harue Seki and her father Nori Seki say their 13 employees largely use Medi-Cal and rely on the emergency room when they get sick.
"We'd really like to be able to offer them health care ... but we can't afford it, Harue Seki said. "It makes it very difficult to compete as a small business owner."
The three women hope California will lead the nation in building the first universal, taxpayer-financed "single payer" health care system independent from the federal government. The state would take over the business of health care, cut out insurance companies and become the sole payer for all services, including primary care, surgeries and prescription drugs.
The idea is not new. Republican Gov. Earl Warren suggested a taxpayer-financed universal health care system in 1945. Voters considered and defeated a version of universal care in 2004. Gov. Arnold Schwarzenegger vetoed a single-payer bill in 2006.
Now there is renewed interest, as proponents like Sen. Kamala Harris and gubernatorial candidate Gavin Newsom see single-payer as the solution to Republican-led efforts to unravel Obamacare. Evidence already shows the law is collapsing under the weight of soaring out-of-pocket costs and fewer affordable coverage options.
As a result, Americans are spending more of their income on medical care, delaying treatments or rationing medicine. Some are opting out of purchasing insurance altogether.
"What happens when our savings is gone? I get scared," Doumas-Toto said. "Democrats in California have a chance to do something about that. They need to be brave."
The idea is being strenuously pushed in the Legislature by the California Nurses Association, but has stalled amid Democratic opposition in the Assembly and is most likely dead for the year. No one has made a detailed proposal with a financing plan. Gov. Jerry Brown is skeptical.
Tremendous uncertainty exists over how a state-based single-payer system would work. No matter how it's crafted, the costs would be steep. Californians likely would face huge increases to their tax bills - both to pay for it initially and to cover inevitable cost increases in the future.
Creating such a system would cost $400 billion per year, more than double the state budget, according to an estimate by the nonpartisan Legislative Analyst's Office, one the nurses dispute.
California taxpayers would be on the hook for at least $200 billion, with the expectation that they would also no longer pay for health care premiums, co-pays or insurance deductibles.
Making that trade-off, both politically and financially, would be difficult to achieve.
On average, a person with private insurance now pays $6,690 a year in premiums, according to the Kaiser Family Foundation.
The estimated tax increases needed to pay for a new system would be unprecedented. Under one scenario, the average statewide sales tax rate would have to jump from 8.5 percent to nearly 37 percent to generate the amount of revenue needed. Under another, California would have to create a new 15 percent payroll tax, withholding $150 from a $1,000-a-week paycheck.
"The tax increases we're talking about are so ridiculously high that you can't assume there wouldn't be significant behavioral responses - people earning less income or leaving the state," said Alan Auerbach, a UC Berkeley economist who directs its Robert D. Burch Center for Tax Policy and Public Finance.
Harue Seki said she'd be willing to pay higher taxes in exchange for single-payer.
"I'm already paying 700 bucks a month for a policy. I'd rather have it be to a state system because the state is not going to have a big profit motive," Seki said. "I've tried private insurance this long, and it's not working. Single-payer wouldn't be perfect, but at least it'd be controlled by a government entity with some public oversight and not a giant corporation."
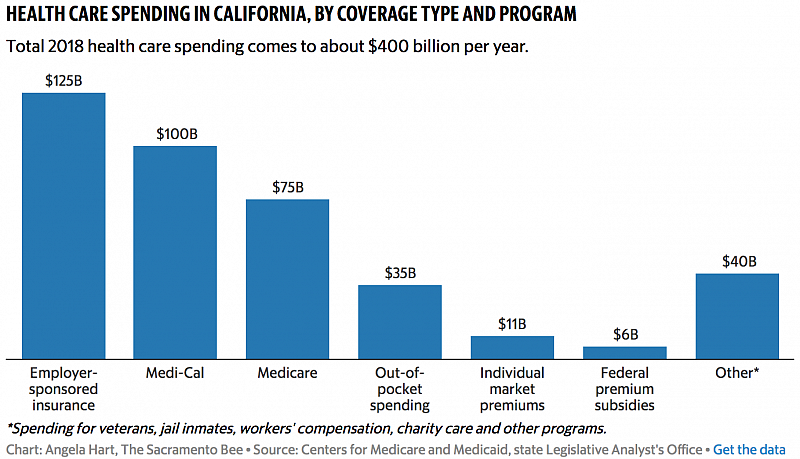
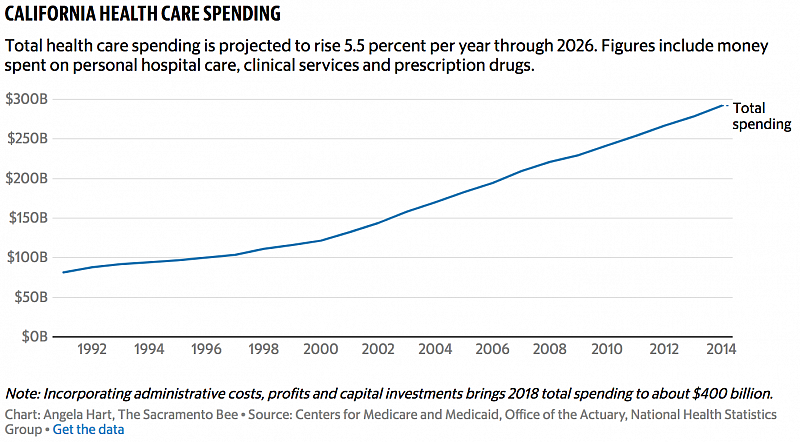
California currently spends roughly $400 billion per year on health care, according to a Sacramento Bee analysis of national health expenditure data from the Centers for Medicare and Medicaid, projections by state health care analysts and independent health economists.
Half of that comes from taxpayers, in the form of federal and state funding for Medi-Cal, the health insurance program for the poor, Medicare for people 65 and older and Covered California premium subsidies. Most of the rest is in the commercial market, with more than 15 million Californians covered through their employers.
To capture the $200 billion in public money currently spent on Medi-Cal, Medicare and federal Covered California subsidies and divert it to a state-based single-payer system, lawmakers would also have to secure numerous federal waivers, legal exemptions to the Affordable Care Act and controversial changes to regulations governing private insurance plans – highly unlikely under President Donald Trump and the Republican-controlled Congress.
Voters would likely have to agree to raise the state's constitutional spending cap and alter the state's school spending guarantee. Two-thirds of lawmakers would have to approve any tax hikes needed to raise $200 billion a year.
Even that might not be enough. Health care costs are continuing to soar, fueled by uncontrolled prices in America's market-driven system.
The state of Vermont learned that lesson when its Democratic governor tried to implementhis version of single-payer four years ago. Former Vermont Gov. Peter Shumlin abandoned his plans in 2014, despite winning majority support from liberal legislators in a deep-blue state that produced Sen. Bernie Sanders, who has championed a national "Medicare-for-all" single-payer plan.
"My critics say I abandoned single-payer because it was too expensive," Shumlin said. "That's not accurate. I abandoned single-payer because health care in America is too expensive. Until we get costs under control, there is no system that we can afford."
"No legislator is going to vote for a system that passes those costs on to consumers in the form of higher taxes," he said. "That's a very tough sell to anyone from any political party."
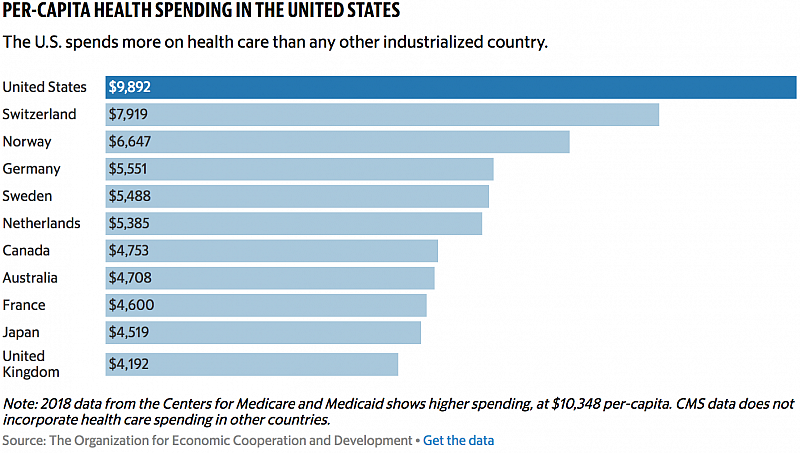
American costs are the highest of the world's industrialized counties.
The United States spent nearly $3.5 trillion on health care last year - more than $10,000 per-capita - and spending is expected to climb 5.5 percent each year from now until 2026, according to the Centers for Medicare and Medicaid.
"Overwhelmingly, the reason we spend so much more is not because we use more health care, but because we pay higher prices in California and across the U.S. – higher prices for drugs, higher prices for hospital care, higher prices for physician care," said Larry Levitt, a health economist and co-executive director for the Program for the Study of Health Reform and Private Insurance at the Kaiser Family Foundation. "Every other country has some kind of government mechanism to control prices."
The Trump administration, meanwhile, is working to dismantle Obamacare and undo regulations put in place under former President Barack Obama aimed at controlling costs, sparking renewed urgency in California for a single-payer system.
"The more Republicans destroy the Affordable Care Act, the more people decide single-payer is what they want," said David Cutler, a health policy expert and professor of economics at Harvard. "People aren't going to say 'Ooh goody, let's let a large share of the population go without health care."
Some see an opportunity for the state to go even further than Obamacare, which doesn't include people like Claudia, the undocumented Pomona mom.
"When I feel pain or something, I just hope it goes away," she said. Claudia is afraid her family will be targeted by an Immigration and Customs Enforcement raid, so The Sacramento Bee agreed to not use her last name. "If I need blood work or I get sick, the first thing that comes to mind is 'I'm going to have to take some money from another bill or rent to pay for it.'"
A single-payer system could cover her, yet without a way to control rising costs, even greater year-over-year tax increases would be required to operate a universal, single-payer system. Unlike the federal government, California cannot operate with a budget deficit.
Major changes to state law would be needed to forestall even greater tax hikes, including deep payment cuts to medical providers, state-regulated caps on total health spending and large-scale transformations in the way providers are paid, to a structure that rewards better health outcomes rather than more care and expensive procedures.
Single-payer proponents argue the government can achieve widespread savings by providing everyone with access to preventive care, negotiating lower provider rates, bulk purchasing of pharmaceuticals and cutting health industry overhead – executive pay, profits, marketing budgets and other administrative costs.
The nurses are convinced those major changes would bring down current costs and control them in the future.
"The reason we take this on is because the health care system has become an industry where money is the metric of good medicine," said Michael Lighty, director of public policy for the nurses association. "Simply providing insurance to everyone will not solve these problems."
Their projections come from University of Massachusetts Amherst economist Robert Pollin, who co-authored a 2017 nurses study on a single-payer bill that stalled in the Legislature last year. The study estimated total spending of $331 billion per year.
No clear consensus concludes how much savings a single-payer system could achieve. But according to more than a dozen experts The Sacramento Bee interviewed, including economists, health care analysts and doctors, some evidence shows that the approach could result in savings.
For traditional Medicare, for example, administrative costs – including advertising, billing and profits – are 1 to 2 percent of total program costs, compared to 11 percent for employer-sponsored insurance and up to 20 percent of for individual insurance, according to an estimate by the Kaiser Family Foundation.
"When you eliminate all that complexity, which is causing all these inefficiencies, you get the biggest chunk of savings," said Jim Kahn, a doctor and professor at the University of California, San Francisco School of Medicine. "When every patient has exactly the same coverage, you get rid of that back-and-forth discussion with insurance companies about 'Why didn't you pay for this, why you didn't pay for that?'"
Still, some argue the savings would not be nearly enough to counter rising costs. The alternative? Rationing care.
"I don't think you can just take it on faith that costs will be controlled," Levitt said. "Otherwise you've got tremendous cost over-runs and taxes have to keep going up, or you've got to cut back on care if you don't have the money to pay for it."
The political hurdles would be monumental, with the insurance industry, pharmaceutical companies and hospitals opposed to the concept. It's already inviting backlash from those who would rather fix the current problems with Obamacare.
A coalition of pharmacy, hospital and doctor groups formed this year to kill any remaining chances to revive a Democratic proposal to create a single-payer system for California. The Coalition to Protect Access to Care includes the California Medical Association, Kaiser Permanente and the California Pharmacists Association, among others.
Members have been meeting with lawmakers and thanking them publicly on Twitter for opposing the single-payer proposal, Senate Bill 562, still languishing in the Legislature. They say they want to #SaveTheACA, and include doctors who ultimately think a single-payer system is the wrong way to go.
Supporters say they may just have to wait for a different governor and a friendly federal administration.
"If you try and change things too fast, it will cause problems and the public won't like it. They'll worry about what will happen with their health insurance," said Stephen Tarzynski, a practicing doctor and president of the California Physicians Alliance. "You want to bring people along with you, not create resentment and opposition."
This article was produced as a project for the USC Center for Health Journalism’s California Data Fellowship.